
This toolkit is also available in Portuguese with Brazilian statistics.
Statistics show that there are very few suicides of children. While this is positive, child suicide deaths are often officially reported as accidents or unintentional deaths so they are likely under-reported (Gray et al., 2014).
Although child suicide deaths are statistically rare, some children do attempt suicide (Whalen et al., 2017). If children with thoughts of suicide are not treated when they are young, their risk of suicide increases as they get older. It is important to identify children thinking about suicide as early as possible so they can receive treatment for mental health concerns (Wyman et al., 2009; Herba et al., 2007).
What to expect
This resource is a brief introduction to the topic of children and suicide. You will learn about statistics, warning signs for suicide, why children may think about suicide, and how these suicides can be prevented. You will also learn how to have a conversation with a child you’re worried about. If you know someone who is actively thinking about suicide and immediately at risk, or if you’re thinking about suicide, call your local crisis line. In Canada, call or text 9-8-8.
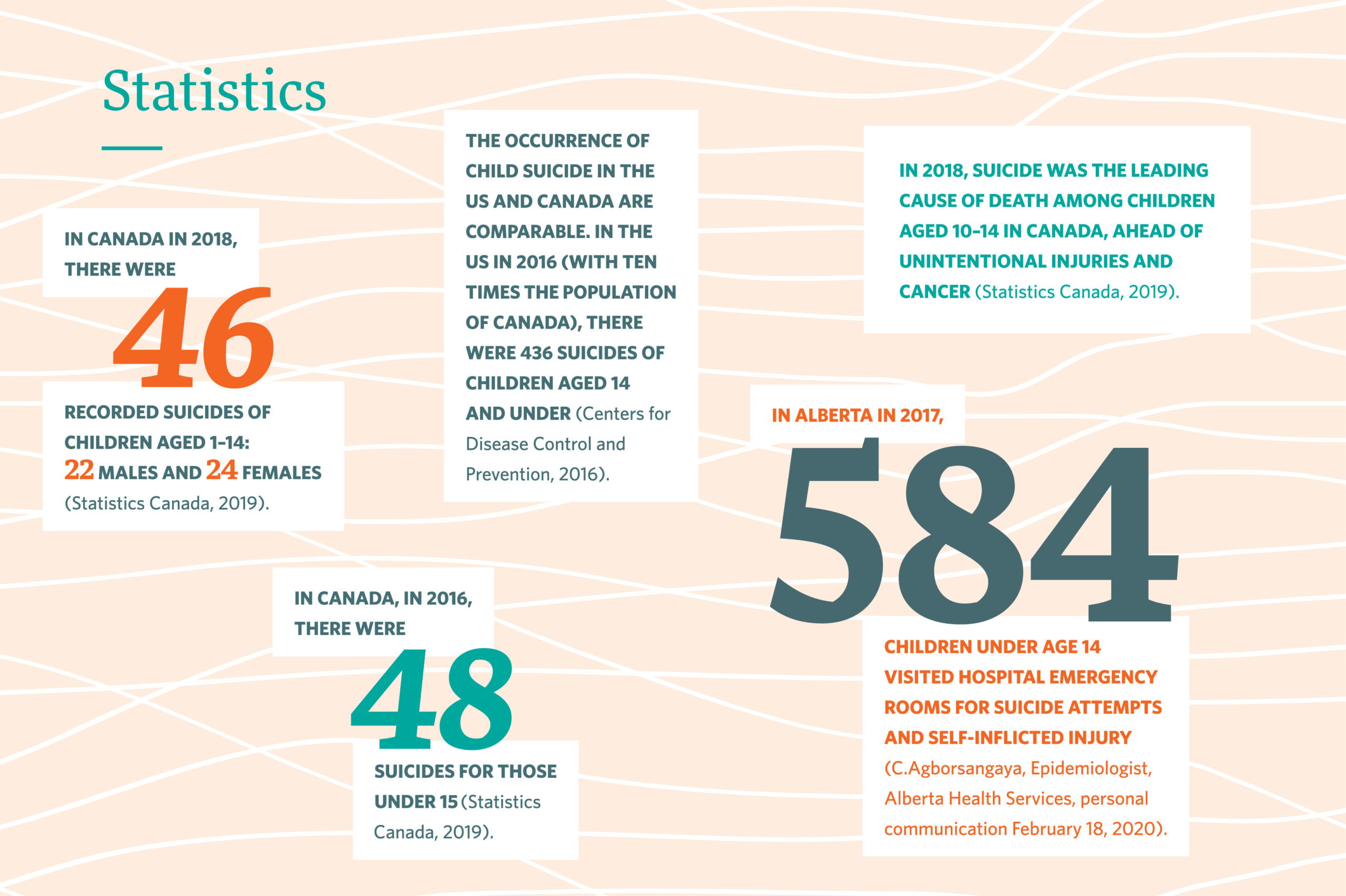
Statistics
Are children really at risk of suicide?
Many people believe that children do not have the developmental maturity to act on suicidal thoughts as they have an incomplete concept of death. However, research shows that by around age 9, many children do have a thorough understanding of both death and suicide (Tishler, 2007; Whalen et al., 2017; Shirley, 2020).
Regardless of whether they understand the consequences of their actions, children may consider death as an option to end their emotional pain without fully understanding the finality of their actions (Tishler, 2007).
Warning signs
People thinking about suicide typically exhibit warning signs – any significant change in behaviour may be a warning sign. Warning signs in children can look like:
- Change in usual behaviour
- Neglecting personal interests or previously enjoyed activities
- Dreaming or worrying about death
- Increasing problems at school, or problems occurring for the first time
- Expressing or demonstrating a general dissatisfaction or disinterest in all activities
(Centre for Suicide Prevention (CSP), 2008, pp. 3, 114-116)
- Risk-taking
- Running into the street
- Climbing buildings or tall trees
- Ingesting inedible material
(Finzi et al., 2001)
- Multiple symptoms of depression
- Experiencing long-term sadness and/or frequent crying
- Developing difficulties concentrating in school
- Losing interest in previously enjoyed activities or lacking energy to participate
- Having insomnia or frequent nightmares
- Routinely not answering questions, or long delays in answering
- Complaining of physical aches and pains not linked to verified illness
- Experiencing anxiety and multiple fears or phobias
- Conversation that indicates suicidal thoughts or plans
- “I’m not very happy most of the time… I think about dying”
- “I think mom left because of me… it would be better if I wasn’t here”
- “I hate my life. I want to go away.”
(CSP, 2008, pp. 3, 114-116)
How to talk to a child about suicide
When talking to a child about suicide:
- Be sensitive to the child’s mood at the beginning of the conversation and notice any changes during the conversation
- Speak slowly, avoid rushing the conversation
- Be aware of their body language as well as what they’re saying
- Maintain an open, non-judgmental tone
- Use clear, direct language
If a child you know is showing warning signs, or you’re just generally worried about them, have a conversation with them:
- Before starting the conversation, decide what role you will play with this child. Will you offer ongoing support? Will you need to tell their caregiver or connect them with supports such as a school counsellor? You can enlist others to help, including your local crisis centre.
- Mention your concerns. “I noticed the other day you said you don’t want to be here because your mom doesn’t live at home anymore. It seems like life is hard for you right now. Are you okay?”
- Listen to their response for expressions of hopelessness, blame, or despair, “It’s my fault that mom left home” or “No… I’m not really okay…”
- You don’t have to offer solutions. Just listen. If you’re concerned after hearing their response, explore further. Ask them about their situation or feelings. Then, if you’re still worried they might be thinking about suicide, ask them directly, “Did you ever feel so upset you wanted to die?” or “Do you think about hurting or killing yourself?” (CSP, 2008, p.35).
- If a child does express thoughts of suicide, let their caregivers know and ensure that child is connected to treatment supports. Your local crisis centre can be used as a resource (in Canada, 9-8-8).
Acute warning signs
Some warning signs require more immediate action than others. If you notice a child exhibiting the following warning signs, call the local crisis line, and, if appropriate, alert the child’s caregiver. If you think the risk of suicide is imminent ensure the child is not left alone – stay with them until they are with a mental health care provider, caregiver, or other contact:
- Talking about wanting to die or kill oneself; and
- Looking for a way to kill oneself or already having a plan (American Association of Suicidology, 2018).
To learn more about how to help a child who is thinking about suicide, consider taking a workshop, such as the half-day Tattered Teddies: Preventing suicide in children or Little Cub: Preventing suicide in Indigenous children workshops. To learn more about suicide intervention, take the two-day ASIST: Applied Suicide Intervention Skills Training.
Risk Factors
Certain factors can place people at a higher risk for suicide than others. These are some risk factors that affect children particularly:
- Family history of suicide, depression, or substance use
- Previous suicide attempts
- Untreated depression, anxiety, or other mental illness
- Incomplete comprehension of death: if a child doesn’t understand the consequences of their actions, they may be more likely to take deadly risks, such as running into traffic, for example
- Self-harm such as repetitively picking wounds, sticking pins into skin, biting fingernails to cause bleeding or pain, self-hitting
- Access to means of suicide such as firearms or prescription drugs
- Learning difficulties or lack of success in school (child may believe they are a failure)
- Exposure to physical, emotional, or sexual trauma
- Unstable home environment resulting from situations such as divorce, frequent moves, or multiple caregivers (child may blame themselves for their circumstances)
- Negative school experiences such as bullying
- Significant recent losses such as the death of a parent, close friend, or pet
(CSP, 2008, pp. 64-79; Tishler, 2007; Whalen et al., 2017; Sheftall et al., 2016.).
Protective Factors
Certain factors or circumstances can guard a person against thinking about suicide and increase their resiliency. These are some protective factors that can build resiliency in children:
- Positive relationships such as with family, teachers, coaches, foster parents, peers
- Positive self-esteem and self-worth
- A hopeful view of the future
- Effective problem solving and coping skills
- Safe and secure home environment
- Positive school experience
- Ability to communicate their needs, feelings, and thoughts to others
- Positive life experiences
- Success at school, sports, or arts activities
- Involvement in faith/religious communities (CSP, 2008, pp. 48-57)

How can suicide in children be prevented?
Positive relationships in a child’s life play a significant role in promoting their mental health and building resilience: they foster self-esteem, competence, and an ability to respond to life’s challenges. Anyone who is in a child’s life can work to build resilience in that child.
At home
Parents and other family members, as well as teachers, coaches, and anyone else who is influential in a child’s life, can take action to build resilience in that child by:
- actively listening, understanding, and validating what they say
- teaching a child that mistakes and problems are opportunities to learn new skills
- identifying and affirming a child’s strengths
- encouraging children to ask for help when it’s needed
(CSP, 2008, pp. 90-91)
At school
Teachers, school counsellors, coaches, and school administrators can all play a role in fostering resilience in children by:
- providing safe, structured, and predictable schedules and routines
- increasing children’s sense of control
- increasing children’s confidence and experience of success by setting achievable goals
- teaching positive behaviours
- ensuring the appropriate response is taken following the suicide death of a student
- implementing suicide prevention programs
(CSP, 2008, pp. 95-97; American Foundation for Suicide Prevention & Suicide Prevention Resource Center, 2018)
Suicide prevention programming in schools is effective when it includes:
- mental health promotion that emphasizes strengths-based activities, resilience and help-seeking
- meaningful student engagement that gives them a sense of belonging and purpose
- training teachers and staff to identify thoughts of suicide in children through gatekeeper training such as the ASIST: Applied Suicide Intervention Skills Training
- easy and apparent access to mental health support at school
- focused and coordinated care following suicide attempts or behaviours that result in hospitalization
(School Mental Health Ontario, 2019)
Resources
Small Talk – Preventing suicide in children workshop
This half-day workshop examines warning signs in a child and intervention strategies.
Little Cub- Preventing suicide in Indigenous children workshop
Little Cub is a one-day, discussion-based workshop examining suicide in Indigenous children and communities.
Reaching Young People – an UK site for ages 6-8 that offers support for children and teaches coping skills for healthy living.
Recommended Reading
To gain a deeper understanding of the complexities of children and suicide, we’ve compiled a recommended reading list on the topic, which is available on our website.
References
American Association of Suicidology. (2018). Know the Warning Signs of Suicide. Retrieved from http://www.suicidology.org/resources/warning-signs
American Foundation for Suicide Prevention, & Suicide Prevention Resource Center. (2018). After a suicide: A toolkit for schools (2nd ed.). Waltham, MA: Education Development Center.
Centre for Suicide Prevention. (2008). Tattered Teddies: An interactive handbook about the awareness and prevention of suicide in children. Calgary: Centre for Suicide Prevention.
Centers for Disease Control and Prevention. (2016). Leading causes of death. Retrieved from https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm
Finzi, R., Ram, A., Shnit, D., Har-Even, D., Tyano, S., & Weizman, A. (2001). Depressive symptoms and suicidality in physically abused children. American Journal of Orthopsychiatry, 71(1), 98-107.
Gray, D., Coon, H., McGlade, E., Callor, W., Byrd, J., Viskochil, J., Bakian, A., Yurgelun-Todd, D., Grey, T. & McMahon, W. (2014). Comparative analysis of suicide, accidental and undetermined cause of death classification. Suicide and Life-Threatening Behaviors, 44(3), 304-316.
Herba, C., Ferdinand, R., van der Ende, J., & Verhulst, F. (2007). Long-term associations of childhood suicide ideation. Journal of the American Academy of Child and Adolescent Psychiatry, 46(11), 1473-1481.
School Mental Health Ontario. (2019). School Mental Health ASSIST: Life Promotion and Suicide Prevention Framework.Author. Retrieved form https://smho-smso.ca/wp-content/uploads/2019/09/Life-Promotion-and-Suicide-Prevention-Framework.pdf
Sheftall, A. H., Asti, L., Horowitz, L. M., Felts, A., Fontanella, C. A., Campo, J. V., & Bridge, J. A. (2016). Suicide in elementary school-aged children and early adolescents. Pediatrics, 138(4), e20160436.
Shirley, K. (2020). Reported trends in suicidality in children 10 and younger. Journal of Mental Health Counseling, 42(1), 47-62.
Statistics Canada. (2019). Table 13-10-0392-01 Deaths and age-specific mortality rates, by selected grouped causes, Canada, annual [CANSIM Database]. Retrieved February 12, 2020 from https://doi.org/10.25318/1310039401-eng
Tishler, C., Reiss, N. & Rhodes, A. (2007). Suicidal behavior in children younger than twelve: A diagnostic challenge for emergency department personnel. Academic Emergency Medicine, 14(9), 810-818.
Whalen, D., Luby, J. & Barch, D. (2017). Highlighting risk of suicide from a developmental perspective. Clinical Psychology Science and Practice, DOI: 10.1111/cpsp.12229.
Wyman, P., Gauderi, P., Schemeelk-Cone, K., Cross, W., Hendricks Brown, C., Sworts, L., West, J., Burke, K. & Nathan, J. (2009). Emotional triggers and psychopathology associated with suicidal ideation in young urban children with elevated aggressive-disruptive behavior. Journal of Abnormal Child Psychology, 37(7), 917-928.