The statistics, research, language, and links used were current when this toolkit was published, but may have become outdated. Please contact us at [email protected] for the most current information, or refer to our newer resources or latest statistics.
Like so many issues in suicide and suicide prevention, military suicide is multi-dimensional and complex – it cannot be easily explained.

Historically, the rate of suicide in the military has been lower than that of the general population. There have been exceptions: the epidemic of suicides that occurred during and after the American Civil War is one instance. Yet, similar epidemics are rare in military environments whether in war or in peace.
Like so many issues in suicide and suicide prevention, military suicide is multi-dimensional and complex – it cannot be easily explained.
Many believe that the American involvement in Iraq and Afghanistan is the direct cause of the heightened suicide rates in the US Army and Marine Corps in recent years (Bush, 2013). The Canadian Forces’ (CF) suicide rate, though, has remained relatively stable over that same period despite the demands of the Canadian mission in Afghanistan. One report shows that even among the suicides that have occurred, there is no direct relationship between deployment in Afghanistan and suicidality (Bogaert et al., 2013).
However, there were multiple suicides in the Canadian military (those on active duty as well as veterans) in the latter part of 2013 and early 2014. Because this is very recent activity, it remains to be seen if this is an anomaly or an indication of an upward trend in CF military suicide.
Statistics
U.S. Military
- In 2008, the Army rate exceeded 20 deaths per 100,000; this was the highest rate in 30 years (Bush, 2013)
- The current rate is 25 deaths per 100,000 (Leenaars, 2013)
- Most military suicides have been white males under the age of 25; 51% were not married; 61% used firearms as their means of suicide (Bush, 2013)
- Some estimates suggest that 15% of American veterans of combat in Iraq and Afghanistan have – or will be diagnosed with – Post Traumatic Stress Disorder (PTSD) (Riggs, 2012)
- A recent study found that, because they felt stigmatized, only 23-40% of those with mental health concerns sought assistance after serving in Iraq and Afghanistan (Regan, 2005)
- 25% of veterans of Operation Iraqi Freedom, and Operation Enduring Freedom in Iraq and Afghanistan have experienced some form of mental health problem (Bryan and Morrow, 2011)
Canadian Forces
CF has an official policy of “universality of service” which dictates that everyone in uniform must be fit and able to be deployed. About 1700 of 4500 soldiers who leave the military every year are deemed “forced release”. This means that they have been forced from the ranks because they no longer qualify as “fit and able” (Campion-Smith, 2014)
Canadian Forces vs General Population
Male Suicides per 100,000
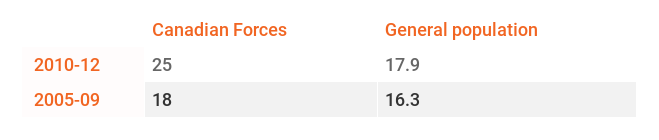
It is important to note that these suicide statistics do not include women, reservists, or veterans. With all subgroups included, the actual numbers are most certainly higher than what the statistics reflect. For example, American veterans are more than twice as likely to die by suicide compared with the general population (Belik, 2009).
Update:
Going forward, veteran suicides will be distinguished from suicides that happen in the general population. A 2017 study of veteran suicide from 1976-2012 has found that Canadian veterans are at a higher risk of dying by suicide than those in the general population.
- Female veterans have a 1.8 times greater risk of suicide
- Male veterans have a 1.4 times greater risk of suicide
(Veterans Affairs Canada, 2017)

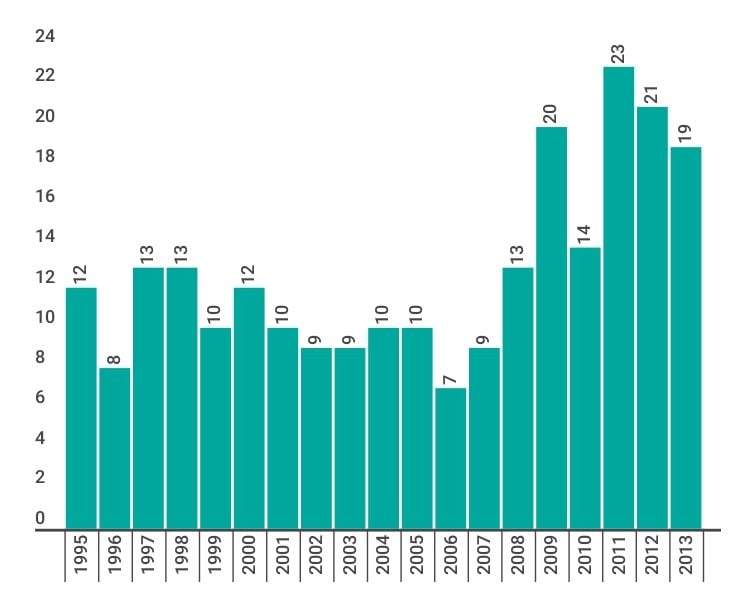
Number of suicides among Canadian Armed Forces personnel
Excerpt
Leenaars envisions the military system as a collective culture; one he characterizes as a “green culture” as opposed to the “blue culture” of the police (10). It is a community that holds such attributes as “Secrecy, stoicism, and denial” (15) as vital to its integrity, which is unsurprising as these are the same traits that some might argue ensure success on the battlefield. The individual is subordinate to the collective, and any behavior which may deviate from that of the model warrior is not tolerated. So what happens, then, if a soldier is traumatized in battle and develops Post Traumatic Stress Disorder (PTSD)? Or what if trauma occurs in another context – such as a military base – and it involves rape or sexual assault? Where is s/he to turn? Confiding in a doctor or therapist can be a career-ending move as there is no expectation of confidentiality. Often military health practitioners receive instructions from the very top to label such soldiers with a personality disorder. Even worse is that this type of disclosure almost always ensured a quick discharge from the military (241). Leenaars correctly asks, “Can the military stoop any lower?” (206).
The stigma that mainstream society has toward mental illness and suicide is brutally magnified in the military setting. This green culture does not encourage help-seeking. The military demands that soldiers adhere to the warrior mentality, and many soldiers would rather die than experience the shame and disgrace that admitting to PTSD or other disorders would bring. It is here that Leenaars repeatedly calls for a more understanding approach by the military. War is indeed trauma, but enduring the intense type of trauma that war brings is atypical of the human experience. Thus, the PTSD reaction is not reflective of a personality disorder, but is, rather, one possible and very common consequence of serving in the military.
The stigma that mainstream society has toward mental illness and suicide is brutally magnified in the military setting.
Leenaars writes passionately about this subject, and emphatically states that things must change! Although his use of language is sometimes informal, his style is refreshingly accessible and he remains at all times authoritative and scholarly. As this is not a typical academic work on suicide it will appeal to and be accessible to anyone with a stake or interest in military suicide.
Early in the book Leenaars presents the “ecological model” of suicide, within which there is no single cause for someone to take his own life, soldier or otherwise. There is no one reason but, rather, a complex interplay of individual, relationship, societal, cultural, and environmental factors; all are contributors (15). Thus, although PTSD may have played a pivotal role in someone’s suicide, there are a host of other factors that could have contributed as well. Traumatic Brain Injury (TBI), for example, is considered a physical trauma but can be a huge risk factor for future suicide as it has also been known to precipitate the psychological symptoms of PTSD (231-233). Another example could be someone with Substance Use Disorder (SUD) abusing drugs or alcohol as a coping strategy to manage depression brought on by spousal loss. These co-occurring disorders put him/her at a greater risk for suicide.
Suicide Among the Armed Forces: Understanding the Cost of Service by Antoon Leenaars (2013). Baywood Publishing Co. 361p.
Risk Factors
- Easy access to firearms
- Longer and more frequent deployments
- Less rigorous screening of new recruits
- Combat trauma
- Presence of mental illness
- Family history of mental disorder
- Substance Use Disorder
- Childhood adversities
- Stressful life events (relationship conflicts, bereavement, legal problems, sexual trauma)
- Lack of access to mental health treatment
- Economic difficulties
- Marital/relationship problems
(Nock et al., 2013; Rozanov et al., 2009; Zamorski et al., 2011; Braswell & Kushner, 2012)

Co-occurring disorders in the military
Some aspects of military service increase the risk of PTSD, depression, and Substance or Alcohol Use Disorder. These are known to be risk factors for suicidality and this risk greatly increases if any of these disorders are co-occurring (Zamorski, 2011).
Post-Traumatic Stress Disorder (PTSD)
PTSD has many psychological symptoms, including:
- Re-experiencing the event
- Avoidance and emotional numbing
- Changes in sleeping patterns
- Hyperarousal (Huckshorn, 2013)
Soldiers and veterans are particularly vulnerable to experiencing PTSD. Combat veterans with PTSD have significantly higher rates of death by suicide than those without PTSD (Bryan, 2013).
PTSD is not reflective of a personality disorder, but is, rather, one possible and very common consequence of serving in the military (Leenaars, 2013).

Substance and Alcohol Use Disorder
- Alcohol Use Disorder has been shown to be extremely prevalent among military populations, at rates 2-3 times the normal population (Belik et al., 2010).
- One survey of American military personnel found that recent trends in heavy alcohol use revealed that males had a high prevalence of binge drinking, up to 45.5% (Sirratt, 2012).
- There is a high co-occurrence of Substance Use Disorder (SUD) and PTSD.
- 20% of veterans diagnosed with PTSD have a co-occurring SUD (Hawkins, 2012).
Traumatic Brain Injury (TBI)
TBI is considered a physical trauma but can be a huge risk factor for future suicide as it has also been known to precipitate the psychological symptoms of PTSD (Leenaars, 2013).
There are two types of TBI:
- Closed Head Injury, which is caused by a blow or jolt to the head that does not penetrate the skull
- Penetrating Head Injury, which occurs when an object goes through the skull and enters the brain.
Soldiers who have experienced a TBI are at greater risk for PTSD, Alcohol and Substance Use Disorder and depression (Sirratt, 2012). The risk of suicide attempts increases after a TBI if the individual also has post-injury psychiatric/emotional disturbance and substance abuse problems (MIRECC, n.d.).
Protective Factors
- Shorter and less frequent deployments
- More rigorous screening of new recruits for mental health concerns
- Social supports
- Psychological protective factors (resiliency, sense of purpose/meaning)
- Access to mental health treatment
(Nock et al., 2013)

In Halifax at the Canadian Association for Suicide Prevention (CASP) conference in 2010, Lieutenant Colonel Rahesh Jetly and Lieutenant Colonel Kenneth Cooper presented a report titled: The Canadian Forces Expert Panel on Suicide Prevention.
Priorities for suicide prevention in military organizations:
- Implement a standard of quality review after each suicide
- Collect more comprehensive information on individual suicides to support future suicide surveillance
- Develop a protocol for mitigating suicide for personnel who are under investigation for legal or disciplinary problems
- Explore opportunities for means reductions for suicides with service firearms and medications
- Engage with the mass media to promote responsible reporting of military suicides
(Zamorski, 2011)
References
Belik, et al. (2010). Are Canadian soldiers more likely to have suicidal ideation and suicide attempts than Canadian civilians? American Journal of Epidemiology, 172(11), 1250-1258.
Bogaert, L., et al. (2013). Suicide in the Canadian Forces, 1995-2012. Retrieved from http://www.forces.gc.ca/assets/FORCES_Internet/ docs/en/about-reports-pubs-health/suicide-in-the-cf-1995-2012.pdf
Braswell, H. and Kushner, H. (2012). Suicide, social integration, and masculinity in the U.S. military. Social Sciences and Medicine, 74(4), 530-536.
Bryan, C., et al. (2013). Combat exposure and suicide risk in two samples of military personnel. Journal of Clinical Psychology, 69, 74-77.
Bryan, C. and Morrow, C. (2011). Circumventing mental health stigma by embracing the warrior culture: Lessons learned from the Defender’s Edge Program. Professional Psychology, 42(1), 16-23.
Bush, et al. (2013). Suicides and suicide attempts in the U.S. military, 2008-2010. Suicide and Life-Threatening Behavior, 43(3), 262-278.
Campion-Smith, B. (2014, February, 21). Soldier suicides “worrying”, Canada’s top general says. Toronto Star. Retrieved from http://www.thestar.com/news/canada/2014/02/21/soldier_suicides_worrying_canadas_top_general_says.html
Hawkins, et al. (2012). Evidence-based screening, diagnosis, and treatment of Substance Use Disorders among veterans and military service personnel. Military Medicine, 177 (8), 29-38.
Huckshorn, K. and Lebel, J. (2013).Trauma-informed care In Yeager, et al. (Eds.) Modern community mental health: An interdisciplinary approach (pp.62-83). Oxford, UK: Oxford University Press.
Leenaars, A. (2013). Suicide among the armed forces: Understanding the cost of service. Amityville, NY: Baywood Publishing.
Mental Illness, Research, Education, and Clinical Center (MIRECC). (n.d.).
Traumatic Brain Injury and Suicide: An Information Manual for Clinicians. Retrieved from http://www.sprc.org/sites/sprc.org/files/ library/TBI_Suicide.pdf
Nock, et al. (2013). Suicide among soldiers. Psychiatry, 76(2), 97-125.
Regan, J., et al. (2005). Suicide and the military. Journal of the Tennessee Medical Association. Retrieved from http://tennessee.gov/ mental/omd/omd_docs/suicideMilitary.pdf
Riggs, et al. (2012). Prevention and care of combat-related PTSD: Directions for future explorations. Military Medicine, 8(14).
Veterans Affairs Canada. (2017). 2017 Veteran suicide mortality study (1976 to 2012). Retrieved from http://www.veterans.gc.ca/eng/about-us/research-directorate/publications/reports/vsms-2017
Rozanov, V., et al. (2009). Suicide in military settings. In Wasserman, D. and Wasserman, C. (Eds.), Oxford textbook of suicidology and suicide prevention: A global perspective (pp.257-265). New York: Oxford University Press.
Sirratt, D., Ozanian, A. and Traekener, B. (2012). Epidemiology and Prevention of Substance Use Disorders in the Military. Military Medicine, 177 (8), 21-28.
Zamorski, M. (2011). Suicide prevention in military organizations. International Review of Psychiatry, 23, 173-180.