
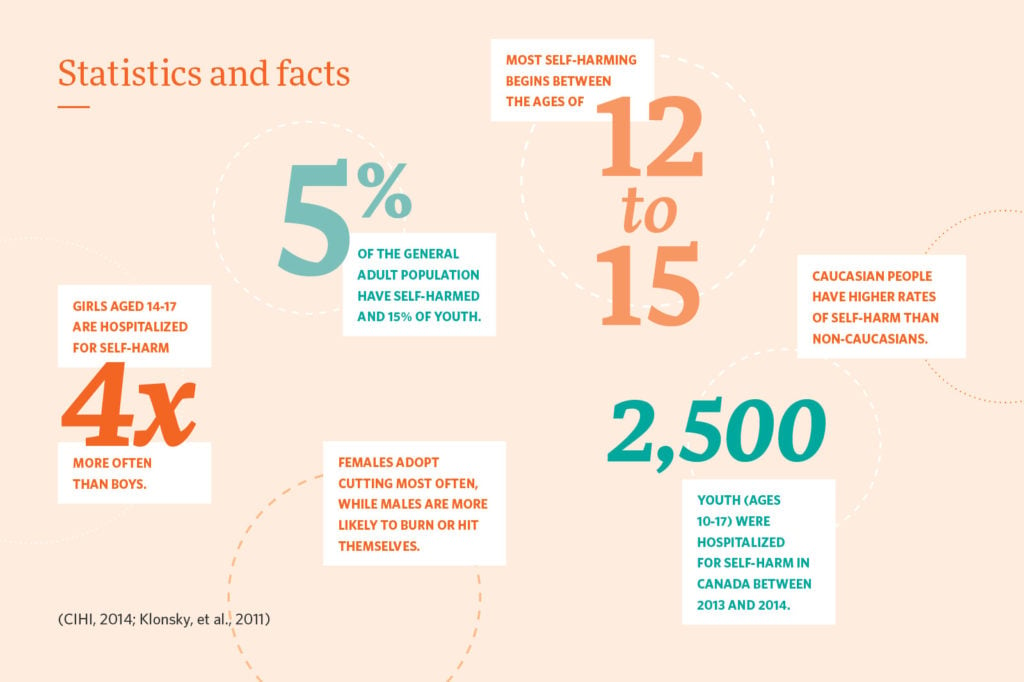
Self-harming behaviours continue to be a major issue in Canada. This is especially true for young people, whose self-harm rates far outnumber those for adults. Self-harm can sometimes be associated with increased suicidality.
Self-harm has been defined as “a preoccupation with deliberately hurting oneself without conscious suicidal intent, often resulting in damage to body tissue” (Muelehkamp, 2005, p.324).
Self-harm does not include tattooing or piercing, or indirect injury such as substance abuse or eating disorders (Self-Injury Outreach and Support [SIOS], n.d.).
Self-harm and Attempted Suicide
Self-harm is also commonly known as self-injurious behaviour (SIB), self-mutilation, non-suicidal self-injury (NSSI), parasuicide, deliberate self-harm (DSH), self-abuse, and self-inflicted violence (Klonsky, 2011).
As one would expect, having multiple terms for self-harm creates misunderstanding and confusion both in academic research and in clinical settings.
Self-harm and suicide attempts can also seem very similar. Sometimes this can result in incorrect treatment assessments (Gratz, 2001).
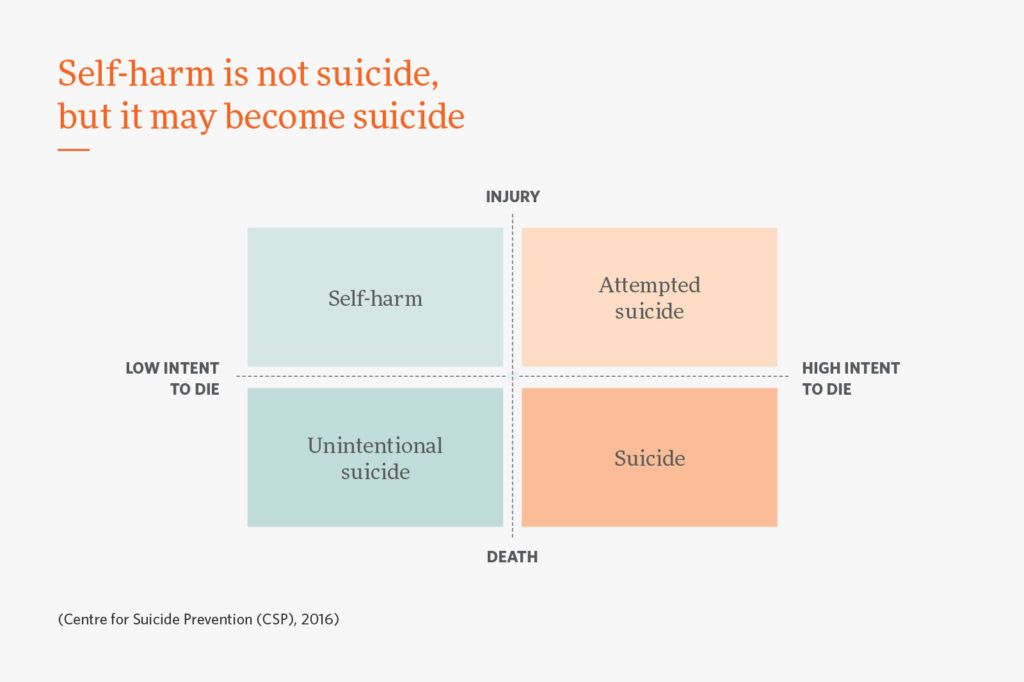
Some researchers classify all forms of self-injury on a suicidal continuum (preceding suicidal ideation), regardless of the victim’s intent. Others emphasize the marked differences between self-harm and attempted suicide, and believe they should be separate areas.

The majority of those who self-injure do not have suicidal thoughts when self-injuring (Klonsky, May & Glenn, 2014).
Although self-harm is not the same as suicide, self-harm can escalate into suicidal behaviours. The intent to die can change over time. One study found that almost half of people who self-harm reported at least one suicide attempt (Klonsky, 2011).
Self-harm can also lead to suicide when:
- Self-harm is no longer an effective coping method. It ceases to offset the feelings caused by stress or trauma (Whitlock & Knox, 2007)
- In a crisis situation, self-harmers who have become desensitized and habituated to pain through repeat harming episodes, may view a suicide attempt as less frightening (Stewart, 2014)
Because self-harm can become suicide, it is highly recommended that every patient who self-harms be assessed for suicide risk (SIOS, n.d.).
Why do people self-harm?
People are more likely be at risk for self-harming behaviours if certain factors are present, such as:
- loss of a parent;
- childhood illness or surgery;
- childhood sexual or physical abuse;
- family substance abuse;
- negative body image perceptions;
- lack of impulse control;
- childhood trauma;
- neglect;
- lack of strong family attachments.
(Briere and Gil, 1998; CSP, 2014)
These risk factors may cause someone to adopt self-harm as a learned coping behaviour to satisfy unmet needs. These behaviours are attempts to compensate for the lack of healthy fulfillment in their lives (CSP, 2014).

People self-harm for a number of reasons, including:
- to feel better
Self-harm can release pent-up feelings such as anger and anxiety, or, people who feel numb use self-harm as a way to feel “something” - to communicate their emotional pain
Those who self-harm for this reason will obviously display their wounds as a way of reaching out for help. - to feel a sense of control
People who self-harm may feel powerless and lack self-esteem. Self-harm may be used as a way to regain control. This is particularly common for those who have suffered abuse. There is often a pronounced feeling of powerlessness, self-loathing, and an absence of self-esteem. - to punish themselves
People who self-harm may lack self-esteem and think they are at fault for the way they feel.
(CSP, 2014; Klonsky and Muehlenkamp, 2007; Hasking, 2010 )
Warning Signs
How can you tell if someone is self-harming?
People who self-harm may:
- appear withdrawn, or more quiet or reserved than usual;
- stop participating in their regular activities;
- have rapid mood changes;
- get angry or upset easily;
- have had a significant event in their lives, e.g. a breakup with significant other;
- suffer poor academic/school performance when they usually do very well;
- exhibit unexplained cuts or scratches;
- wear clothes that are inappropriate for the weather, e.g. wearing long sleeves on hot day.
(Hasking, 2010; SIOS, n.d.)
What to say and what to do if someone you know is self-harming
- Ask how they are feeling.
- Do not be judgmental.
- Be supportive without reinforcing their behaviour.
- Educate yourself about self-harm.
- Acknowledge their pain.
- Do not promise confidentiality.
- Do not avoid the subject.
- Do not focus on the behaviour itself.
- Encourage them to seek professional help.
(CMHA, 2013; CSP, 2014)
Treatments
Self-harm is treatable.
Cognitive Behaviour Therapy (CBT) is a psychological therapy that aims to address issues such as anxiety and depression, as well as a range of other mental health concerns. It helps someone become aware of inaccurate or negative thinking, so challenging situations can be seen more clearly and responses to them are more effective.
Dialectical Behaviour Therapy (DBT) is a variation of CBT treatment designed for individuals with self-harming behaviours, such as self-cutting, suicidal thoughts, and suicide attempts (Sanderson, 2008). The focus of DBT is to help a person change behaviours that may be self-destructive – such as self-harm – and work toward a more fulfilling life.
Problem Solving Therapy (PST) is a brief psychological intervention that focuses on identifying the specific problems that an individual is facing, and generating alternative solutions to these problems. Individuals learn to clearly define a problem that they face, brainstorm multiple solutions, and decide on the best course of action (Hasking, 2010; CIHI, 2014; Sanderson, 2008).
Resources
S.A.F.E (Self Abuse Finally Ends) Alternatives
A U.S. based treatment approach, professional network, and educational resource base which is committed to helping to achieve an end to self-injurious behaviours.
www.selfinjury.com
Self-Injury Outreach and Support (SIOS)
SIOS is a non-profit outreach initiative providing information and resources about self-injury to those who self-injure, those who have recovered, and those who want to help.
www.sioutreach.org
References
Briere, J. & Gil, E. (1998). Self-mutilation in clinical and general population samples: Prevalence, correlates and functions. American Journal of Orthopsychiatry, 68(4), 609-620.
Canadian Institute for Health Information. (2014). Intentional self-harm among youth in Canada. Retrieved from https://www.cihi.ca/web/resource/en/info_child_harm_en.pdf
Centre for Suicide Prevention. (2016). Straight Talk: Youth Suicide Prevention Workshop. Calgary, AB.: Author.
Centre for Suicide Prevention. (2014). The 5 things we wish all teachers knew about: Self-harm and suicide. Retrieved from https://connect.srv.ualberta.ca/p5rd64xyc0t/?launcher=false&fcsContent=true&pbMode=normal
Grantz, K. (2001). Measurement of deliberate self-harm: Preliminary data on the Deliberate Self- Harm Inventory. Journal of Psychopathology and Behavioral Assessment, 23(4), 253-263.
Hasking, M., et al. (2010). Seeking solutions to self-injury: A guide for young people. Brisbane, Australia: Centre for suicide prevention studies, The University of Queensland.
Joiner, T. (2005). Why people die by suicide. Cambridge, MA.: Harvard University Press.
Klonsky, E., et al. (2011). Nonsuicidal Self-Injury. Toronto, ON. : Hogrefe Publishing.
Klonsky, E., May, A. & Glenn, C. (2014). The relationship between nonsuicidal self-injury and attempted suicide: Converging evidence from four samples. Journal of Abnormal Psychology, 122(1), 231-237.
Muehlenkamp, J. (2005). Self-injurious behavior as a separate clinical syndrome. American Journal of Orthopsychiatry, 75(2), 324-333.
Sanderson, C. (2008). Dialectical Behavior Therapy frequently asked questions. Retrieved from http://behavioraltech.org/downloads/dbtFaq_Cons.pdf
Self-Injury Outreach and Support.(n.d.). SIOS: A guide for school professionals. Retrieved from http://www.insync-group.ca/publications/SiOS_School_Professionals.pdf
Stewart, S., Baide, P. & Theall-Honey, L. (2014). Examining non-suicidal self-injury among -adolescents with mental health needs in Ontario, Canada. Archives of Suicide Research, 18(4), 392-409.
Whitlock, J. & Knox, K. (2007). The relationship between self-injurious behavior and suicide in a young adult population. JAMA Pediatrics, 161(7), 634-640.