September 11, 2017
Editorial
Aiming for Perfection: The Zero Suicide Movement
Robert Olson, BA, MLIS, Librarian & Writer, Centre for Suicide Prevention
infoExchange is an original resource that examines topics relating to suicide in a way that encourages conversation, written in an editorial style.

There is a movement within healthcare systems striving to eliminate suicide. Fittingly, it is called the Zero Suicide Movement. When I first heard this name a couple of years ago, I did a double-take. This is a bold statement, arguably, an unattainable one. Why would a program purport to achieve what it could not possibly deliver? Is it dangerous to make a promise that simply cannot be kept? Can suicide really be eradicated like polio? I wondered if such a movement was doomed to fail from the very start.
Upon closer scrutiny, however, the name and claim of Zero Suicide began to make more sense. There are many other industries that have set seemingly lofty goals of achieving perfect safety records. As such, over the past three decades the airline, auto, nuclear power, and construction industries, among others, have dramatically improved their safety records. Each organization began their quest for safety perfection by first setting that exact goal: zero. They wrote it into their official company directives, set it as an expectation, developed concrete strategies to set the new trajectory and over time it became fully embedded in workplace culture. Which brings us to today, where it is now commonplace to view perfection as a goal. We expect our flights to not crash-land and our bridges to not collapse. Healthcare is no exception. Over the last couple of decades, we have seen significant uptake in patient safety and have redesigned systems to better prevent untoward events. Why then, are we reluctant to apply this same principle to suicide? If suicide is indeed preventable, can we not also make changes in practice to drive our suicide rate to zero?
There are many reasons why we may think Zero Suicide is a non-starter and, arguably, these reasons are grounded in our values and beliefs. Historically, suicide has been viewed as an unfortunate negative outcome of some other mental health concern. Suicide is scary: we often do not want to talk about it for fear of inciting it, offending someone, or being at a loss of how to thwart it. It is still not uncommon today for people to say that people determined to kill themselves eventually will, they believe there is ultimately nothing we can do to stop them. This is a myth: suicide is preventable, because people considering suicide do not actually want to die: they want the pain of living to end. The Zero Suicide movement posits that suicide is in and of itself a mental health concern and should be addressed directly. It is predicated on the belief that suicide is preventable, and that people can recover from suicidal crisis.
A patient presenting at an emergency room for suicidality should be stabilized – people in suicidal crisis cannot sustain this crisis point for long – it is either resolved by intervention or death. Stabilization is key but it is not the only treatment needed: it is equally important that any co-occurring concerns (such as depression, anxiety, substance use disorder or a particular psychosis) are fully recognized, as they may be underlying their suicidality.
Sadly, we hear many stories of patients being discharged from hospital emergency rooms once “stabilized” only to die by suicide on their way home: their suicide risk has not been fully addressed. Others may make it home from the hospital but do not return for follow-up. In the US, approximately 70% of patients who leave the emergency room after a suicide attempt fail to attend their first follow-up appointment (Luxton, et al., 2013). This is alarming. Why and how is our system failing these vulnerable people? How can we create wrap-around care to support people considering suicide?
Origins
In the 1990s, there was growing discontent with the seemingly rampant negligence found in US healthcare systems. Up to 98,000 deaths per year in the US occurred because of medical errors, ranking medical errors in the top 10 causes of deaths. 20% of suicide deaths were by people who had been treated by the healthcare system and then discharged (de Jonge, et al., 2011).
Healthcare leaders examined the quality assurance approach used in the airline industry, among others, for inspiration (de Jonge, et al., 2011). Quality of care, service, and safety measures needed to be assessed, improved, and embedded in healthcare systems. Medication errors and emergency room negligence were two areas that required immediate attention. But what about the needless suicide deaths among both inpatients and outpatients? Could the prevention, intervention, and postvention of suicides be treated in similar ways as all other quality standards in healthcare?
The Institute of Medicine (IOM) published a landmark document in 1999 called To err is human: Building a safe health system. This declaration outlined several steps to improve quality and safety in healthcare, and called for the implementation of protocols, projects, and legislation that focused on medical errors (de Jonge, et al, 2011).
One of the steps suggested was to introduce the Sentinel Event Policy to ensure inpatient safety. This policy detailed how to increase patient awareness, establish a culture of safety, and implement and monitor effective patient safety strategies. Sentinel events are the harms (including death) that happen to patients that are not related to their illness or underlying condition. These are not just the physical mistakes that result from malpractice or negligence, but also those that can affect the patient’s mental health, for example, the trauma that can be experienced within the hospital environment. Once these events are evaluated, corrective actions are taken to avoid repeat occurrences.
Despite the implementation of the Sentinel Event Policy, suicide deaths in hospital settings did not cease. So, in 2016 a continuation of the original policy was issued which aimed to assist all healthcare organizations to better identify and treat patients with suicidal ideation (Hogan & Grumet, 2016). This was a definitive and necessary step forward in mental health care. We still have work to do though: in 2004, 19% of all errors occurred within behavioural health settings, compared to 5.4% within emergency rooms and 0.9% within private practice (Jabbarpour, 2016).
Henry Ford Healthcare System
When the IOM published their document back in 1999, they chose 12 organizations across the US to demonstrate their recommendations on “healthcare re-design” (Hampton, 2010). The Henry Ford Healthcare System (HFHCS) in the US was the only behavioural health organization (their focus was on depression and anxiety) to participate. In 2001, HFHCS created a Perfect Depression Care program that addressed depression through 6 specific areas: safety, effectiveness, patient-centeredness, timeliness, efficiency, and equity. Although there are often direct correlations between depression and suicide, the program still achieved unexpected results – suicides were reduced from 89 per 100,000 to 22 in the first four years. In the following two years, they had no suicides at all. The news of these very promising results travelled fast, and became the impetus to strive for “no suicide” as a permanent goal (Hampton, 2010).
As I stated earlier, this idea of eliminating suicides completely may raise expectations to an unreasonable and, ultimately, disappointing level. Clinicians and staff may view this goal as intimidating, and, thus, experience a great fear of failure. When accidents happen – as they always do – healthcare system employees may feel that they will be targeted as scapegoats. Therefore, a culture of “blaming and shaming” may result.
A quality assurance approach proposed by the Zero Suicide movement, however, deals with this issue: errors are classified as “system errors” as opposed to “human errors”. Although it is recognized that mistakes happen because humans make them, individuals are not considered at fault because it is either the system itself or a flaw within it that is to blame. All errors are examined in a system-wide context, and evaluated to identify the root cause. Adjustments are then made to avoid future failure (de Jonge, et al., 2011). Ultimately, the onus of responsibility is on the entire system, not the individual.
The United States Air Force
As the healthcare industry began these actions towards quality assurance, the US military implemented the first-ever systems-wide suicide prevention program. It was called the Air Force Suicide Prevention Initiative (1996–2002), and it had a huge impact on suicide rates within its ranks. One of the mandates of the program was that all members receive suicide intervention skills and information training. All members were strongly encouraged to look out for each other’s mental well-being, learn how to identify someone considering suicide or in distress, and locate resources if they identify someone in need. They called this practice “buddy care,” and it was intended to alleviate fear of reprisals from high-ranking officers because of possible lingering stigma surrounding mental health issues. Airmen relied on one another for peer support, but there was also a strong commitment of leadership from personnel at the top to ensure that the culture of suicide prevention was strongly endorsed and sustained. From 1997 to 2003, the suicide rate dropped by 33%. This early example of dedicated efforts to lessen or eliminate suicides within a closed system was a successful demonstration of how focusing on suicide directly can achieve positive results (Knox, et al., 2010).
Magellan
Magellan of Arizona, a Health Maintenance Organization (HMO) in the US, also made serious progress addressing suicide within their system. In the early 2000s, they realized that many of the deaths occurring in their care were suicides. Major system weaknesses were revealed in their 2009 review, when they discovered that there was little to no continuity of care for their patients who had experienced a suicidal crisis; they were often discharged after initial emergency treatment without follow-up of any kind. They determined that this lack of follow-up was indirectly causing suicides. It was also revealed that there was a belief among the organization’s clinicians that crisis intervention and suicide prevention were viewed as secondary elements – not core elements of patient care. Additionally, no connection was being made between a patient’s presenting acute suicidal symptoms and their underlying mental health concerns.
Following the review, suicide intervention skills training was mandated for all their 2100 employees, working in 30 locations. Magellan administrators also created a new clinical care model, implemented a system-wide approach, and added several new topics to their training program, including attempt survivor peer support, family engagement, community integration, and racial/ethnic best practices. In 2009, they officially launched The Programmatic Suicide Deterrent System, and their reduction of suicidal deaths reached an outstanding 38% by the end of 2011 (Grantham, 2011).
The Zero Suicide Initiative
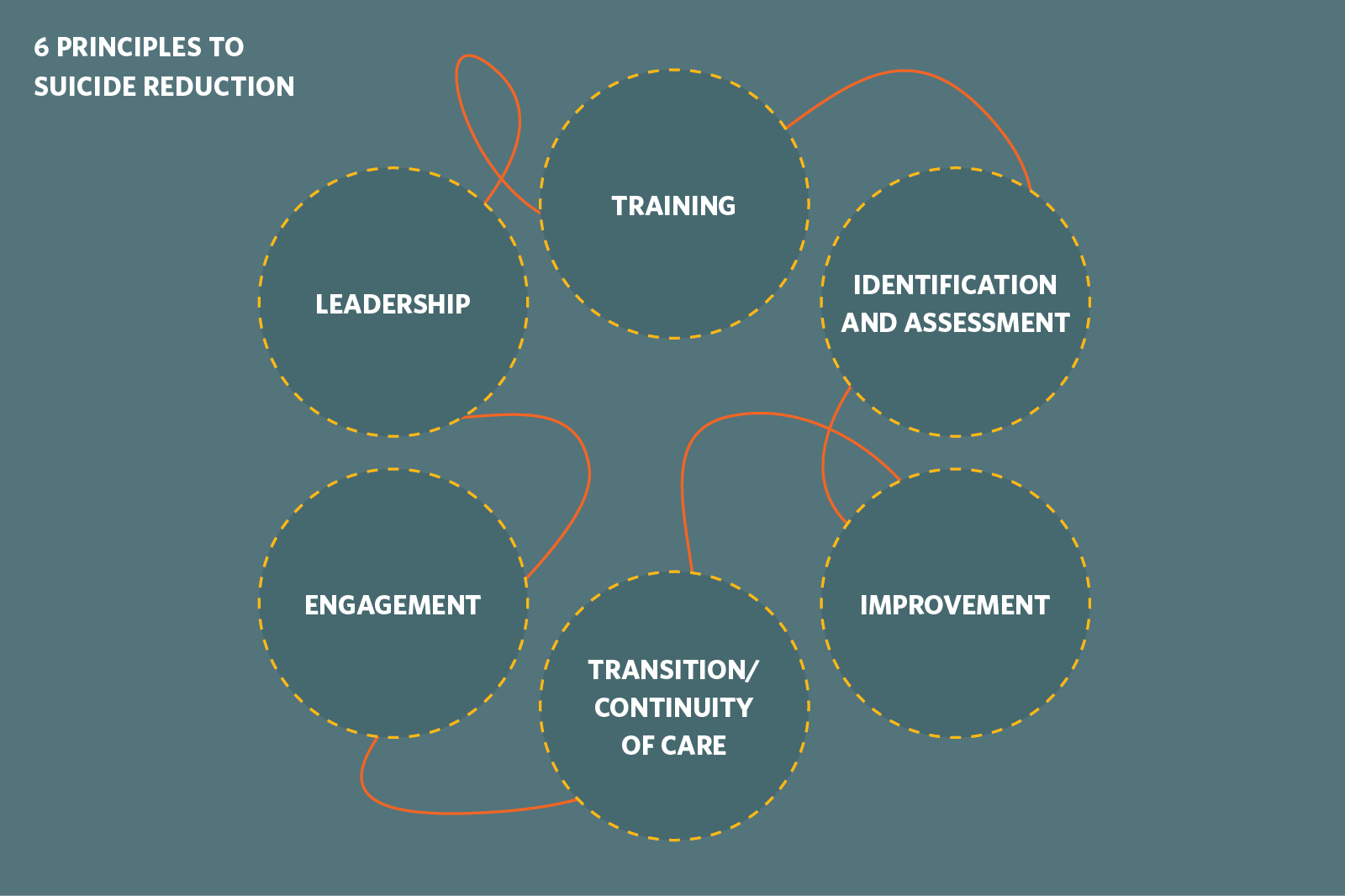
These examples prove that a systematic approach to eliminating suicide can achieve results. The next big step forward came in 2012 when the National Alliance for Suicide Prevention (NASP) formed the Clinical Care and Intervention Task Force to codify some of these elements into what became known as the Zero Suicide Initiative. The task force looked at Henry Ford, Magellan, the Air Force Suicide Prevention Program, and the National Suicide Prevention Lifeline, and determined that there are six pillars needed to successfully reduce suicidal deaths across a system. These are: leadership, training, identification and assessment, engagement, treatment, transition/continuity of care, and improvement (Educational Development Centre, 2015). Read more about it here: http://zerosuicide.sprc.org/
These 6 pillars together form the foundation of the Zero Suicide initiative.
Along with the Suicide Prevention Resource Centre (SPRC), NASP unveiled the Zero Suicide Initiative: a program that provides a transferable, system-wide approach to improve outcomes and bridge existing gaps in healthcare systems. They felt that any organization with strong leadership in place could effectively deal with the issue of suicide. Their hope was that this prescribed approach would gather traction and be replicated throughout the US and the world.
IIMHL Conference
Fast-forward to the September 2015 International Initiative for Mental Health Leadership (IIMHL) and International Association for Suicide Prevention (IASP) conference. In Atlanta, Georgia, mental health experts from thirteen nations came together to craft a formal declaration for reaching the goal of Zero Suicide in healthcare – to make suicide a “never event.” These experts included leaders with lived experience of suicide loss and attempted suicide, healthcare management and policy, as well as suicide prevention experts in public health, private health, and community care. This conference introduced the Zero Suicide movement internationally, and broadcast to the world both its accomplishments and future possibilities.
Read about it here: https://riinternational.com/wp-content/uploads/2016/03/zerosuicidedeclaration_2015draft.pdf
More recent successes, both in North America and abroad, include:
Centerstone America
In Nashville, Tennessee, Centerstone America saw a 65% decrease in their suicide rate from 31 per 100,000 to 11 per 100,000 in a 20-month period after implementing Zero Suicide. It was also determined that a savings of $440,000 accrued annually because of reduced emergency room visits and hospitalizations.
Mersey Care
In the UK one of the most promising programs was developed in 2015 by Mersey Care, who called their initiative “Quality, recovery, and well being at the heart of everything we do.” In addition to the core elements of the Zero Suicide program, Mersey Care’s program includes post-suicide reviews within 72 hours of an event, personalized safety plans for anyone with a suicidal or self-harm history or future intent, and a “Safe from Suicide Team” that responds and intervenes more rapidly and effectively for those considering suicide. Read more: http://www.merseycare.nhs.uk/about-us/striving-for-perfect-care/our-zero-suicide-initiative/
Here is a recent article by the Manchester Guardian describing Mersey Care’s Zero Suicide’s efforts: https://www.theguardian.com/society/2017/aug/01/zero-suicide-the-bold-new-fight-to-eradicate-suicide

St. Joseph’s Hospital
Canada unveiled its first Zero Suicide campaign in May 2016 at the St. Joseph’s Healthcare Foundation in London, Ontario. This quality assurance initiative “set a bold, aspirational goal of reducing suicides and attempted suicides for individuals within our mental health program, and eventually throughout the London area.” Following a pilot period, there is a plan to extend the program to other hospitals in London.
To date, some 200 healthcare and behavioural heath organizations have implemented Zero Suicide initiatives, and many more have proposed to adopt similar programs soon. I believe that this movement will continue to gather momentum as more centres and organizations become familiar with the concept, and see the benefits of its sound objectives.
While the future is hopeful, today there are still many distressing factors faced by suicidal patients regarding their treatment. Patients considering suicide are often discharged in the name of “efficiency,” which is both cruel and unethical: it jeopardizes the opportunity for patients to undergo a complete assessment of their suicidality. This is especially disheartening because the risk of suicide is three times higher the week following a hospital discharge (Bickley, et al., 2013). Also, within institutional walls there are still approximately 1500 inpatient suicides in the US every year (Jabbapour, 2016). Stigma must be addressed among care providers to create an opportunity for a change in values and beliefs. Only once people believe that recovery from suicidality is possible can new systems be implemented to better prevent suicide deaths. Further, within a healthcare system, a suicidal death must be attributed to a flaw in the system, not to an individual, thus, it is the culture within that system that must change.
Driving hospital suicides to zero is only the beginning. The vast majority of suicide deaths do not occur in the healthcare system at all. Most suicides occur at an individual’s home – in secrecy, and far under the radar or influence of any healthcare facility (Harvard School of Public Health, 2017).
This is why the Zero Suicide movement is even more important: it shows that in a closed system, a zero-“accident” rate can be achieved and it promotes the idea that we can help those who are suicidal.
Canada’s Landscape
The initiative created at St. Joseph’s in Canada is a promising start, but more widespread and committed efforts need to be taken. Anecdotal reports abound regarding the substandard care being administered to psychiatric patients across the country. A CTV news investigation found that over ten years 330 suicides occurred in Canadian hospitals, which did not even factor in those suicides that occurred after discharge.
In Alberta, we have experienced our share of failures within our own healthcare system. The most egregious examples are those involving individuals who present at the emergency room for suicidality being discharged right away, or being admitted then released without suitable follow-up. Too often this neglect has resulted in suicide. Training staff in suicide prevention equips them to recognize that a suicidal patient could be displaying symptoms of other disorders. They would know that an appearance in an emergency room and then a quick stint in psychiatric care is often not the most effective way to support a person considering suicide. For many people, an inpatient stay is only one phase in a complex recovery journey. In a perfect system, hospital clinicians would recognize the complexities of suicide and be more finely attuned to the unique needs of each patient. Acute care would work seamlessly with community care to provide long-term support for our most vulnerable. But it all begins with what we believe about suicide: can it be prevented? Can people recover from suicidal crisis? Or is it an unfortunate eventuality for 4000 Canadians annually?
Imagine a community where people no longer assume that we will always have suicide, where all suicide attempts are thwarted, where people get the help they need when they need it.
Zero Suicide is “a bold goal and an aspirational challenge” (Educational Development Center, 2015) but it is not fiction: it’s already being implemented in healthcare systems and communities in the western world. Positioning suicidality as a priority, rather than an unfortunate possible outcome of something else, Zero Suicide challenges our thoughts and beliefs about suicide prevention and people in crisis. This paradigm shift, that we can learn to prevent suicide across the board, is taking off. And we want to see it here in Alberta.
We at the Centre for Suicide Prevention know that this is possible. People who work with individuals in crisis want to see them heal, grow, and manage their challenges so they can lead constructive lives. We endorse the Zero Suicide movement in hospital settings but it cannot stop there. If the stigma of suicide erodes and the view that one suicide is too many takes hold in greater society, then a benchmark goal of no suicides is also conceivable. Truly, it is all about values and beliefs. As more of us realize that recovery from chronic suicidality is possible and this belief is further supported by acute care, community care, government agencies, advocacy groups, and the public at large, then the ideal of eliminating suicide altogether becomes increasingly possible. Over time, this combined effort will become embedded in our collective Canadian culture.
To start with, though, a more focused and concerted approach to suicidality needs to be implemented by our provincial healthcare systems, who need to stand up and bear responsibility for these preventable deaths. Adopting a program like Zero Suicide is the proper next step. Dr. Edward Coffey, an architect of the Zero Suicide movement asked, “If zero is not the right number, what is?” We emphatically agree that zero is, indeed, the right number.
References
Bickely, H., Hunt, I., Windfurh, K., Shaw, J., Appleby, L. & Kapur, N. (2013). Suicide within two weeks of discharge from inpatient care: A case-control study. Psychiatric Services, 64(7), 653-659.
de Jonge, V., Nicolaas, J., van Leerdam, M. & Kuipers, E. (2011). Overview of the quality assurance movement in healthcare. Clinical Gastroenterology, 25(3), 337-347.
Education Development Center. (2015). Zero Suicide in health and behavioral healthcare. Retrieved from www.zerosuicide.com
Grantham, D. (2011). New perspectives on suicide prevention. Behavioral Healthcare, 31(4).
Hampton, T. (2010). Depression care effort brings dramatic drop in large HMO population’s suicide rate. Journal of American Medical Association, 303(19), 1903-1905.
Harvard School of Public Health. (2017). Where do suicides occur? Retrieved from https://www.hsph.harvard.edu/means-matter/basic-suicide-facts/where/
Hogan, M. & Grumet, J. (2016). Suicide Prevention: An emerging priority for healthcare. Health Affairs, 35(6), 1084-1090.
Jabbapour, Y. (2016). Suicide prevention in healthcare. Focus: The Journal of Lifelong Learning in Psychiatry, 14(2), 222-224.
Knox, K., Pflanz, S., Talcott, G., Campise, R., Lavigne, J., Bajorska, A., Xin, T. & Caine, M. (2010). The US Air Force Suicide Prevention Program: Implications for public health policy. American Journal of Public Health, 100(12), 2457-2463.
Luxton, D., June, J., Comtois, K. (2013). Can postdischarge follow-up contacts prevent suicide and suicidal behavior? A review of the evidence. Crisis, 34(1), 32-41.
Mersey Care NHS Foundation Trust. (2017). Our zero tolerance approach to suicide prevention. Retrieved from http://www.merseycare.nhs.uk/about-us/striving-for-perfect-care/our-zero-tolerance-approach-to-suicide-prevention/